Endodiabology 2004; Issue 1 (February)
ENDODIABOLOGY
NORTHEAST NEWSLETTER
FOR SPRs AND BOSSES TRAPPED IN THE NORTHERN DEANERY
February 2004
Editors: Shahid Wahid and Petros Perros
Associate Editors: Peter Carey and Freda Razvi
SpR PLACEMENTS (NTN/VTN year of training from 1st October 2003)
RVI- David Woods(4), Rahul Nayar(3), Peter Carey(2), Sony Anthony(2), Gerry McKay, Faisal Al-Terkait
Freeman- Kamal Abouglila(4), Simon Ashwell(3), Stella Kaddis(3/4)
North Tyneside/Wansbeck- Arun/SME Al-Sabagh
South Tyneside- Andrew Advani(2)
Gateshead- Dr Bhatacharya
Sunderland- Tom Barber(2)
North Tees/Hartlepool- , Laura Chapman/ E Lin Lim(1)
Middlesbrough- Ronan Canavan(5), Liz McIntyre(5), Arutchelvan Vijayaraman
Carlisle-
Bishop Auckland- Rafe Al-Mohammed
NGH-E Al-Ozairi
Research with numbers (supervisor)- Latika Sibal (Prof Home), Salman Razvi (Dr Weaver), B Ravikumar (Prof Taylor), Ibrahim M Ibrahim (Prof Walker), Akheel Syed (Dr Weaver), Sath Nag (Dr Connolly), Reena Thomas (Dr Shaw), Mutu Jayapaul (Prof Walker)
MEETINGS / LECTURES / ANNOUNCEMENTS
25th February 2004 Society for Endocrinology Clinical Cases meeting, London. Contact Ann Lloyd
26th February 2004 Northern Endocrine & Diabetes Winter CME, Freeman Hospital. Contact Ronan Canavan
11th March 2004 Clinical Endocrinology Trust Lecture Lecture by Professor Wiersinga, University of Newcastle, Medical School, Demonstration theatre, 4th Floor Catherine Coockson Building, 1500-1745. Contact Petros Perros
16th March 2004 Young Diabetologists Forum, Birmingham. Contact Camilla Bull
17th-19th March 2004 Diabetes UK annual professional conference, Birmingham. Contact Diabetes UK
22nd-24th March 2004 23rd Joint British Endocrine Societies annual professional conference, Brighton. Contact Society for Endocrinology
24th March 2004 GIM SpR training ½ day, Sunderland Royal. Contact Lorraine Waugh 0191 223 1247
31st March-2nd April 2004 Osteoporosis and other metabolic bone disease: a course for SpRs, Oxford. Contact Tamara Lloyd
31st March 2004 NoReN-early detection and treatment of diabetes, Millfield Conference Centre, Pets Corner, Jesmond Dean, Newcastle, 1315-1630. Contact Gilian Hawthorne or Noren Network
1st April 2004 Deadline for Abstracts for 12th International Congress for Endocrinology, Lisbon, August 31st-4th September 2004.
29th April 2004 Novo Nordisk Lecture. Professor Rury Holman. Newcastle General Hospital, 1730. Contact Sally Marshall
5th May 2004 Northern Region Diabetes Service Advisory Group meeting followed by the Audit meeting, Collingwood Centre, Durham. Contacts Jola Weaver, or Shahid Wahid
7th-8th May 2004 European Diabetic Nephropathy Study Group meeting, Bergamo, Italy. Contact Roberto Trevisan
12-14th May 10th Malvern Diabetic Foot Conference, Manchester. Contact Anne Roscoe
25th May 2004 GIM SpR training ½ day, Freeman Hospital. Contact Lorraine Waugh 0191 223 1247 Lorraine Waugh
27th May 2004 Northern Endocrine & Diabetes Summer CME, Freeman Hospital. Contact Ronan Canavan
4-8th June 2004 American Diabetes Association Conference, Orlando, Florida, USA. Contact The ADA
16-19th June 2004 ENDO 2004, New Orleans, USA. Contact Beverly Glover
5th July 2004 GIM SpR training ½ day, Sunderland Royal. Contact Lorraine Waugh 0191 223 1247
TRAINING ISSUES
Diabetes Extra-curricular activities As part of obtaining a rounded-broad range of training it is strongly recommended that trainees involve themselves with some of the activities run by Diabetes UK. There is a Children's Support Holiday at Frontier Centre, Northamptonshire (11-15 years old) on 7-14 August 2004. Further details of all care support events and application forms can be requested from Diabetes UK on 020 7424 1000, e-mail Diabetes UK, Diabetes UK events
Audit Trainees are constantly asked about audit during their training. Trainees are expected to have completed at least 3 “significant” audit projects during their training. Feeding back the results of an audit are essential. Currently the annual Endocrine meeting at Lumley Castle provides an excellent forum for presenting Endocrine audits. Audits in Diabetes can be presented at the Northern Region Audit meetings (following the NRDSAG) held biannually in early May and October. When planning audits I would suggest that completion be timed for around these periods so that an application to present the audit results can be submitted to the Regional Audit Lead for the NRDSAG. For further information please contact Shahid Wahid
Mentoring A small group recently met to discuss introducing a mentoring scheme. It was decided categorically that longitudinal educational supervision (one of the major suggestions by the SAC on how our training programme could be improved) and mentoring are NOT the same thing. Jean MacLeod has recently presented a scheme whereby the region could introduce a longitudinal education supervision scheme. Further information will be circulated shortly. There are plenty of merits for the region adopting a mentoring scheme. The first that needs to happen is that Trainees and Trainers are educated about what mentoring actually is and also some training needs to be provided for folk in mentoring skills. Watch this space ….
SPARROWS GSK will continue to sponsor up to 4 trainees who wish to attend the ADA in June 2004. This is an excellent opportunity. For further details please contact Jean Macleod
Training Committee Regional Speciality Advisor- Mark Walker; Committee Chairman- Petros Perros; Programme Director- Richard Quinton; Consultant member- Jola Weaver ; Consultant member- Jean Macleod ; SpR representatives- Simon Ashwell & Andrew Advani
NEW FACES ON THE SCENE
Welcome to Eelin Lim, who has recently obtained a training number in the region. She is currently at Hartlepool and North Tees and will be rotating in to the centre from October 2004.
Nick Quinn an SpR in Leeds has been appointed as the second Consultant at Friarage Hospital with Roger Fisken. He will also have some sessions at James Cook University Hospital in Middlesbrough. He will officially start on 1st April 2004. A more official welcome will be given in the next Newsletter.
OLD FACES ON THE GO
David Fryer Has left the region for Australia. He has his CCST and no doubt will be on the look out for a new job on his return.
Alison Gallagher has obtained her CCST and plans to take a break travelling before taking the plunge for a Consultant post.
Liz McIntyre is planning to act up as a Consultant in Wansbeck.
Umesh Dashora has left for Southampton to begin his Training Number.
Abdul Suliman has obtained a Consultant post in Ireland and will be leaving Hartlepool soon.
NEWS FROM THE NORTHEAST
Congratulations to Ronan Canavan on his Consultant appointment at Sunderland Royal from April 2004.
Andrew Advani has joined the training committee as the second SpR representative.
Congratulations to Andrew Advani for obtaining his PhD and on the birth of his baby daughter.
Congratulations to Richard Quinton on the birth of his baby daughter.
Congratulations to Sony Anthony, Reena Thomas and Mutu Jayapaul on obtaining their Training Numbers in the region.
Congratulations to Kamal Abouglila and Steve Ball on having their case accepted for oral presentation at the annual Society for Endocrinology Clinical Cases meeting.
There is a new rotational slot on the SpR Training Programme at The University Hospital of North Durham, with Eric Saunders as the Educational Supervisor.
Freda Razvi is on maternity leave.
LETTERS
Contributions for this section can include meeting reports, research experiences, book reviews, experiences abroad, and anything else you feel may benefit trainees and trainers around the region. The success of this section really does depend on YOU.
BOOK REVIEW-Shaz Wahid
Management of Diabetic Nephropathy. Eds. Bonner G and Cooper ME. Martin Dunitz, London & New York, 2003.
This is an excellent read that covers everything form aetiopathogenesis to treatment for both Type 1 and 2 diabetes related diabetic nephropathy. Through out the book the use of a MRFIT and multidisciplinary team approach to managing patients with diabetic nephropathy was very evident, with an excellent summary chapter on treatment co-authored by Rudy Bilous and Steve Jones. The only gripes that I have are with the rather disappointing chapters that dealt with patients with end-stage renal disease. Very little coverage was given to the practical management of such patients, eg insulin administration via the peritoneal route in CAPD patients, the effects of dialysis on glucose control and how to manage them. However, overall I would recommend this book for both trainers and trainees.
LIFE ON THE OTHER SIDE-Sarah Frewin
For those of you who don’t know me, I'm Sarah, a Clinical Nurse Specialist in Endocrinology. For the last 7 years I’ve worked with Petros Perros at the Freeman Hospital in Newcastle. I had a fantastic time working with Petros and all you registrars who have happened through the Freeman during my time, but in February last year things changed dramatically for me. I was dispatched by the Trust to do a prescribing course to help me run my clinics in a more efficient way. Over the past few years Petros had tried to encourage me to apply to go to medical school but I had always resisted, not believing that I was bright enough and convincing myself nursing was my lot in life. This course changed my opinion not only of my own abilities but also of nursing in general. One of the tutors on the course made a comment one day that nurses could convert to medicine in four years. I had never appreciated this, and the seed was sown. I spent the next few weeks in turmoil trying to decide whether I should apply or not. For a start I didn’t know whether I would even be accepted or meet the selection criteria. On top of that there were the financial implications of leaving my job and going back to full time study. After a few sleepless nights I eventually broached the subject with Petros hoping he would bring me back to my senses. “Well I told you to do it years ago” were his words and the rest’s a whirlwind. My husband was ecstatic about the idea and vowed to find the money come what may, as I was to be his new pension plan. Before I knew it I was being interviewed for a place in the course at Durham’s Stockton campus.
The interview was quite possibly one of the most emotional experiences I have ever had, not knowing what to expect, what they were looking for and it meaning so much to me. I was interviewed in May of last year and told that I could have a place on the reserve list as all the places were taken. Well I was devastated but not deterred, I vowed to hang on until the A level results came out. A level results came and went but still no news. I began to hound them with daily phone calls and eventually at the end of August the call came to say I had a place. I now know what it must feel like to be a contestant on pop Idol. When I got the call all I could do was say thank you, thank you, thank you. The course leader must have thought I was a blithering idiot!
Knowing what I know now however, the interview was the easy part; it was the first month or so that challenged me more than anything ever before. Anyone who tells you nursing stands you in good stead for medicine is sadly misguided! I spent the first few weeks thinking any day now they’ll teach me something I already know, but alas it was never to be! I truly believed that with ten years nursing and two degrees under my belt it would be a breeze and I would be able to opt out of lots of lessons. Oh how deluded I was!
The first four weeks constituted the ‘Foundation Course’ aimed at getting all students up to the same level in terms of human and cell biology. I didn’t do science at school and nursing tends to skim over these issues. The fact that chromosomes were actually scrunched up DNA was an absolute revelation to me I’m embarrassed to say and don’t get me started on protein folding! So the Foundation Course, which was supposed to be the easy part was one of he most difficult things I've ever done. One of my new friends, Claire was a molecular cell biologist before medical school, spent endless hours with play-dough chromosomes teaching me about mitosis and meiosis. In fact in retrospect within the first few weeks of the course there was nothing that I didn’t struggle with. I never once questioned whether I had made the right decision but did occasionally wonder if I could cut the mustard.
I struggled through the Foundation Course only to be met head on by Cardio Vascular, Respiratory and Renal Medicine (CVRRM). The Foundation Course suddenly paled into insignificance beside it, but at last a session I had been waiting for, measurement of Blood Pressure arrived. One session from which I could at last opt out, however I ended up having to help out as a demonstrator for the rest of the students! Its not all a hard slog, lots of the course is aimed at the more ‘touchy feely’ side of medicine which is right up my street. Lots of the other students are struggling with the social science, research and clinical skills side of things but these come relatively easily to me because of my nursing background and previous degrees. I’ve also discovered an affinity for physiology, which I never expected, perhaps because of the fantastic way it has been taught and the enthusiasm of the teacher.
Well the first exams (formative) were in November and I passed, I’m relieved to say. I didn’t come top of the year by any stretch of the imagination but I was happy with the results and they renewed my self-belief that I really can do it. So I’m sitting here writing this with six days to go until my first proper summative exams, make or break time, hopefully make!
I’d like to take this opportunity to thank all the people who have supported me, encouraged me and kept me calm over the past year. In particular I would like to thank Petros for his unwavering belief in me and all his help with the application forms and interview, I couldn’t have done it without him. Also Raz Nayar for his friendship and encouragement when I was going to give up on applying and since, his time sacrifices in helping me get through my exams.
Roll on the summer holidays, for all of you who have forgotten about the delights of university holidays……. four months off!
RECENT PUBLICATIONS FROM THE NORTHEAST
Please send us your recent publication for inclusion in the next newsletter.
1. Ball SG, Barber T, Baylis PH. Tests of posterior pituitary function. J Endocrinol Invest. 2003;26:15-24.
2. Ball SG, Barber TM. Molecular development of the pancreatic beta cell: implications for cell replacement therapy. Trends Endocrinol Metab. 2003;14:349-55.
3. Dashora U, Mathias D, James A, Zammit-Maempel I, Perros P. Management of recurrent pituitary cysts with pituitary-nasal drain. Pituitary 2003, 5:225-233.
4. Harding S, Greenwood R, Aldington S, Gibson J, Owens D, Taylor R, Kohner E, Scanlon P, Leese G; Diabetic Retinopathy Grading and Disease Management Working Party. Grading and disease management in national screening for diabetic retinopathy in England and Wales. Diabet Med. 2003;20:965-71.
5. Hart RH, Perros P. Glucocorticoids in the medical management of Graves' ophthalmopathy. Minerva Endocrinol. 2003;28:223-31.
6. Hawthorne G, Irgens LM, Lie RT, Moe N, Jervell J. Retraction of paper on maternal diabetes. BMJ. 2003;327:929.
7. Krassas GE, Perros P. Thyroid disease and male reproductive function. J Endocrinol Invest 2003;26:372-380
8. Marshall SM. Inhibition of the renin-angiotensin system: added value in reducing cardiovascular and renal risk? Diabet Med. 2004;21:1-3.
9. Perros P, Mallick UK, Fenwick JD. Radioiodine Uptake in Normal Female Breasts and Liver of a Patient with Differentiated Thyroid Cancer Imaged by Whole Body Scanning. Thyroid 2003; 13, 511.
10. Phillips AW, Fenwick JD, Mallick UK, Perros P. The impact of Clinical guidelines on surgical management of thyroid cancer. Clin Oncol 2003, 15:485-489.
11. Rawling LD, Advani A, Marshall SM, Thomas TH. Neutrophil antigen exposure is altered with age in relatives of patients with Type 2 diabetes. Diabetologia. 2003 Dec 10 [Epub ahead of print]
12. Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R. Medical therapy of macroprolactinomas in males: I. Prevalence of hypopituitarism at diagnosis. II. Proportion of cases exhibiting recovery of pituitary function. Pituitary. 2003;10:243-6.
13. Syed AA, Irving JAE, Redfern CPF, Hall AG, Unwin NC, White M, Bhopal RS, Alberti KGMM, Weaver JU. Low prevalence of the N363S polymorphism of the glucocorticoid receptor in South Asians living in the United Kingdom. Journal of Clinical Endocrinology & Metabolism 2004, 89(1), 232-235
14. Syed AA, Weaver JU. Insulin resistance and coronary artery disease: body mass index may have affected results. Diabetes, Obesity and Metabolism 2004, 6(1), 78
15. Syed AA. Invisible oedema. Journal of the Royal College of Physicians of Edinburgh 2003, 33, 295-296
16. Syed AA. What is a good death?: A good death follows a good life. BMJ 2003, 327(7422),1047
17. Syed AA, Evans C, Ludgate M, Lazarus JH. Early changes in thyroid stimulating antibody activity following radioiodine therapy. Medical Principles and Practice 2003, 12(4), 266-268.
18. Taylor R. Conundrum of the HOPE study: time of taking ramipril may account for lack of relation between blood pressure and outcome. BMJ. 2003;327:681-2
19. Weightman DR, Mallick UK, Fenwick JD, Perros P. Discordant serum thyroglobulin results generated by two classes of assay in patients with thyroid carcinoma: correlation with clinical outcome after 3 years of follow-up. Cancer 2003; 98:41-7.
20. Patel S, Woods DR, Macleod NJ, Brown A, Patel KR, Montgomery HE, Peacock AJ.Angiotensin-converting enzyme genotype and the ventilatory response to exertional hypoxia. Eur Respir J. 2003 Nov;22(5):755-60.
21. Woods D, Sanders J, Jones A, Hawe E, Gohlke P, Humphries SE, Payne J, Montgomery H. The serum angiotensin-converting enzyme and angiotensin II response to altered posture and acute exercise, and the influence of ACE genotype. Eur J Appl Physiol. 2003; 6:821-896.
RECENT PUBLICATIONS IN DIABETES & ENDOCRINOLOGY THAT HIT THE NEWS OR THAT MAY HAVE A SIGNIFICANT IMPACT ON MANAGEMENT
Withdrawal of long-term cabergoline therapy for tumoural and nontumoural hyperprolactinaemia. Colao A, Di Sarno A, Cappabianca P, Di Somma C, Pivonello R, Lombardi G. N Engl J Med. 2003 Nov 20;349:2023-33.
This important observational and prospective trial looked at whether the withdrawal of treatment in patients with nontumouralhyperprolactinaemia, microprolactinomas, or macroprolactinomas is safe and effective. The study population included 200 patients--25 patients with nontumoral hyperprolactinaemia, 105 with microprolactinomas, and 70 with macroprolactinomas. Withdrawal of cabergoline was considered if prolactin levels were normal, magnetic resonance imaging (MRI) showed no tumour (or tumour reduction of 50% or more, with the tumour at a distance of more than 5 mm from the optic chiasm, and no invasion of the cavernous sinuses or other critical areas), and if follow-up after withdrawal could be continued for at least 24 months. Recurrence two to five years after the withdrawal of cabergoline was 24% in patients with nontumoural hyperprolactinaemia, 31% for microprolactinomas and 36% for macroprolactinomas. Renewed tumour growth did not occur in any patient; in 10female patients (22%) and 7 male patients (39%) with recurrent hyperprolactinaemia, gonadal dysfunction redeveloped. In all diagnostic groups, prolactin levels at the time of recurrence were significantly lower than at diagnosis (Pless than 0.001). The Kaplan-Meier estimated rate of recurrence at five years was higher among patients with macroprolactinomas and those with microprolactinomas who had small remnant tumours visible on MRI at the time of treatment withdrawal than among patients whose MRI scans showed no evidence of tumour at the time of withdrawal (patients with macroprolactinomas, 78% vs. 33%, P=0.001; patients with microprolactinomas, 42% vs. 26%, P=0.02). In conclusion, cabergoline can be safely withdrawn in patients with normalised prolactin levels and no evidence of tumour. However, because the length of follow-up in this study was insufficient to rule out a delayed increase in the size of the tumour, it is essential that patients be closely monitored.
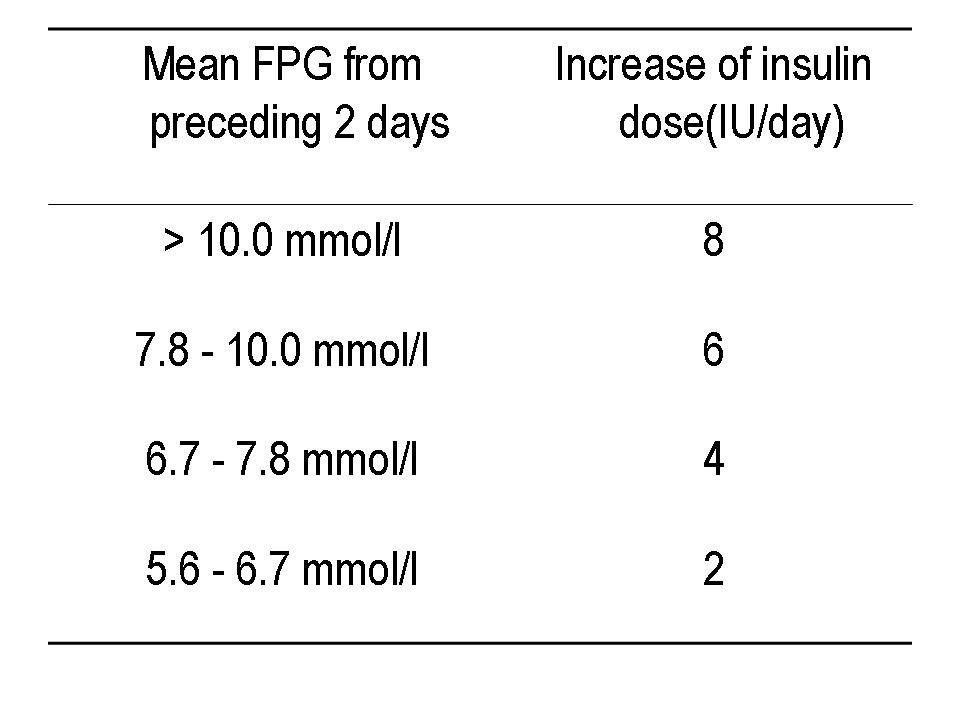
The treat-to-target trial: randomised addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators.
This randomised, open-label, parallel, 24-week multicentre trial compared the abilities and associated hypoglycaemia risks of insulin glargine and human NPH insulin added to oral therapy of type 2 diabetes to achieve a target HbA1c of 7%. 756 overweight men and women with inadequate glycaemic control (HbA1c more than 7.5%) on one or two oral agents continued their prestudy oral agents and received bedtime glargine or NPH once daily, titrated using a simple algorithm (see table) seeking a target fasting plasma glucose (FPG) less than 5.5 mmol/l.
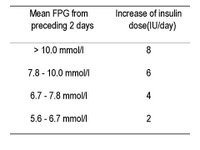 The mean FPG at end point was similar with glargine and NPH (6.5 vs. 6.7 mmol/l), as was HbA(1c) (6.96 vs. 6.97%). 60% of patients attained HbA1c less than 7% with each insulin type. However, nearly 25% more patients attained this without documented nocturnal hypoglycaemia (less than 4.0 mmol/l) with glargine (33.2 vs 26.7%, P less than 0.05). Moreover, rates of other categories of symptomatic hypoglycaemia were 21-48% lower with glargine. In conclusion, systematically titrating bedtime basal insulin added to oral therapy can safely target HbA1c in a majority of overweight patients with type 2 diabetes with HbA1cbetween 7.5 and 10.0% on oral agents alone. In doing this, glargine causes significantly less nocturnal hypoglycaemia than NPH, thus reducing a leading barrier to initiating insulin. This simple regimen may facilitate earlier and effective insulin use in routine medical practice, improving achievement of recommended standards of diabetes care.
The mean FPG at end point was similar with glargine and NPH (6.5 vs. 6.7 mmol/l), as was HbA(1c) (6.96 vs. 6.97%). 60% of patients attained HbA1c less than 7% with each insulin type. However, nearly 25% more patients attained this without documented nocturnal hypoglycaemia (less than 4.0 mmol/l) with glargine (33.2 vs 26.7%, P less than 0.05). Moreover, rates of other categories of symptomatic hypoglycaemia were 21-48% lower with glargine. In conclusion, systematically titrating bedtime basal insulin added to oral therapy can safely target HbA1c in a majority of overweight patients with type 2 diabetes with HbA1cbetween 7.5 and 10.0% on oral agents alone. In doing this, glargine causes significantly less nocturnal hypoglycaemia than NPH, thus reducing a leading barrier to initiating insulin. This simple regimen may facilitate earlier and effective insulin use in routine medical practice, improving achievement of recommended standards of diabetes care.
NEXT NEWSLETTER Due out beginning of June 2004, so keep the gossip coming.
NORTHEAST NEWSLETTER
FOR SPRs AND BOSSES TRAPPED IN THE NORTHERN DEANERY
February 2004
Editors: Shahid Wahid and Petros Perros
Associate Editors: Peter Carey and Freda Razvi
SpR PLACEMENTS (NTN/VTN year of training from 1st October 2003)
RVI- David Woods(4), Rahul Nayar(3), Peter Carey(2), Sony Anthony(2), Gerry McKay, Faisal Al-Terkait
Freeman- Kamal Abouglila(4), Simon Ashwell(3), Stella Kaddis(3/4)
North Tyneside/Wansbeck- Arun/SME Al-Sabagh
South Tyneside- Andrew Advani(2)
Gateshead- Dr Bhatacharya
Sunderland- Tom Barber(2)
North Tees/Hartlepool- , Laura Chapman/ E Lin Lim(1)
Middlesbrough- Ronan Canavan(5), Liz McIntyre(5), Arutchelvan Vijayaraman
Carlisle-
Bishop Auckland- Rafe Al-Mohammed
NGH-E Al-Ozairi
Research with numbers (supervisor)- Latika Sibal (Prof Home), Salman Razvi (Dr Weaver), B Ravikumar (Prof Taylor), Ibrahim M Ibrahim (Prof Walker), Akheel Syed (Dr Weaver), Sath Nag (Dr Connolly), Reena Thomas (Dr Shaw), Mutu Jayapaul (Prof Walker)
MEETINGS / LECTURES / ANNOUNCEMENTS
25th February 2004 Society for Endocrinology Clinical Cases meeting, London. Contact Ann Lloyd
26th February 2004 Northern Endocrine & Diabetes Winter CME, Freeman Hospital. Contact Ronan Canavan
11th March 2004 Clinical Endocrinology Trust Lecture Lecture by Professor Wiersinga, University of Newcastle, Medical School, Demonstration theatre, 4th Floor Catherine Coockson Building, 1500-1745. Contact Petros Perros
16th March 2004 Young Diabetologists Forum, Birmingham. Contact Camilla Bull
17th-19th March 2004 Diabetes UK annual professional conference, Birmingham. Contact Diabetes UK
22nd-24th March 2004 23rd Joint British Endocrine Societies annual professional conference, Brighton. Contact Society for Endocrinology
24th March 2004 GIM SpR training ½ day, Sunderland Royal. Contact Lorraine Waugh 0191 223 1247
31st March-2nd April 2004 Osteoporosis and other metabolic bone disease: a course for SpRs, Oxford. Contact Tamara Lloyd
31st March 2004 NoReN-early detection and treatment of diabetes, Millfield Conference Centre, Pets Corner, Jesmond Dean, Newcastle, 1315-1630. Contact Gilian Hawthorne or Noren Network
1st April 2004 Deadline for Abstracts for 12th International Congress for Endocrinology, Lisbon, August 31st-4th September 2004.
29th April 2004 Novo Nordisk Lecture. Professor Rury Holman. Newcastle General Hospital, 1730. Contact Sally Marshall
5th May 2004 Northern Region Diabetes Service Advisory Group meeting followed by the Audit meeting, Collingwood Centre, Durham. Contacts Jola Weaver, or Shahid Wahid
7th-8th May 2004 European Diabetic Nephropathy Study Group meeting, Bergamo, Italy. Contact Roberto Trevisan
12-14th May 10th Malvern Diabetic Foot Conference, Manchester. Contact Anne Roscoe
25th May 2004 GIM SpR training ½ day, Freeman Hospital. Contact Lorraine Waugh 0191 223 1247 Lorraine Waugh
27th May 2004 Northern Endocrine & Diabetes Summer CME, Freeman Hospital. Contact Ronan Canavan
4-8th June 2004 American Diabetes Association Conference, Orlando, Florida, USA. Contact The ADA
16-19th June 2004 ENDO 2004, New Orleans, USA. Contact Beverly Glover
5th July 2004 GIM SpR training ½ day, Sunderland Royal. Contact Lorraine Waugh 0191 223 1247
TRAINING ISSUES
Diabetes Extra-curricular activities As part of obtaining a rounded-broad range of training it is strongly recommended that trainees involve themselves with some of the activities run by Diabetes UK. There is a Children's Support Holiday at Frontier Centre, Northamptonshire (11-15 years old) on 7-14 August 2004. Further details of all care support events and application forms can be requested from Diabetes UK on 020 7424 1000, e-mail Diabetes UK, Diabetes UK events
Audit Trainees are constantly asked about audit during their training. Trainees are expected to have completed at least 3 “significant” audit projects during their training. Feeding back the results of an audit are essential. Currently the annual Endocrine meeting at Lumley Castle provides an excellent forum for presenting Endocrine audits. Audits in Diabetes can be presented at the Northern Region Audit meetings (following the NRDSAG) held biannually in early May and October. When planning audits I would suggest that completion be timed for around these periods so that an application to present the audit results can be submitted to the Regional Audit Lead for the NRDSAG. For further information please contact Shahid Wahid
Mentoring A small group recently met to discuss introducing a mentoring scheme. It was decided categorically that longitudinal educational supervision (one of the major suggestions by the SAC on how our training programme could be improved) and mentoring are NOT the same thing. Jean MacLeod has recently presented a scheme whereby the region could introduce a longitudinal education supervision scheme. Further information will be circulated shortly. There are plenty of merits for the region adopting a mentoring scheme. The first that needs to happen is that Trainees and Trainers are educated about what mentoring actually is and also some training needs to be provided for folk in mentoring skills. Watch this space ….
SPARROWS GSK will continue to sponsor up to 4 trainees who wish to attend the ADA in June 2004. This is an excellent opportunity. For further details please contact Jean Macleod
Training Committee Regional Speciality Advisor- Mark Walker; Committee Chairman- Petros Perros; Programme Director- Richard Quinton; Consultant member- Jola Weaver ; Consultant member- Jean Macleod ; SpR representatives- Simon Ashwell & Andrew Advani
NEW FACES ON THE SCENE
Welcome to Eelin Lim, who has recently obtained a training number in the region. She is currently at Hartlepool and North Tees and will be rotating in to the centre from October 2004.
Nick Quinn an SpR in Leeds has been appointed as the second Consultant at Friarage Hospital with Roger Fisken. He will also have some sessions at James Cook University Hospital in Middlesbrough. He will officially start on 1st April 2004. A more official welcome will be given in the next Newsletter.
OLD FACES ON THE GO
David Fryer Has left the region for Australia. He has his CCST and no doubt will be on the look out for a new job on his return.
Alison Gallagher has obtained her CCST and plans to take a break travelling before taking the plunge for a Consultant post.
Liz McIntyre is planning to act up as a Consultant in Wansbeck.
Umesh Dashora has left for Southampton to begin his Training Number.
Abdul Suliman has obtained a Consultant post in Ireland and will be leaving Hartlepool soon.
NEWS FROM THE NORTHEAST
Congratulations to Ronan Canavan on his Consultant appointment at Sunderland Royal from April 2004.
Andrew Advani has joined the training committee as the second SpR representative.
Congratulations to Andrew Advani for obtaining his PhD and on the birth of his baby daughter.
Congratulations to Richard Quinton on the birth of his baby daughter.
Congratulations to Sony Anthony, Reena Thomas and Mutu Jayapaul on obtaining their Training Numbers in the region.
Congratulations to Kamal Abouglila and Steve Ball on having their case accepted for oral presentation at the annual Society for Endocrinology Clinical Cases meeting.
There is a new rotational slot on the SpR Training Programme at The University Hospital of North Durham, with Eric Saunders as the Educational Supervisor.
Freda Razvi is on maternity leave.
LETTERS
Contributions for this section can include meeting reports, research experiences, book reviews, experiences abroad, and anything else you feel may benefit trainees and trainers around the region. The success of this section really does depend on YOU.
BOOK REVIEW-Shaz Wahid
Management of Diabetic Nephropathy. Eds. Bonner G and Cooper ME. Martin Dunitz, London & New York, 2003.
This is an excellent read that covers everything form aetiopathogenesis to treatment for both Type 1 and 2 diabetes related diabetic nephropathy. Through out the book the use of a MRFIT and multidisciplinary team approach to managing patients with diabetic nephropathy was very evident, with an excellent summary chapter on treatment co-authored by Rudy Bilous and Steve Jones. The only gripes that I have are with the rather disappointing chapters that dealt with patients with end-stage renal disease. Very little coverage was given to the practical management of such patients, eg insulin administration via the peritoneal route in CAPD patients, the effects of dialysis on glucose control and how to manage them. However, overall I would recommend this book for both trainers and trainees.
LIFE ON THE OTHER SIDE-Sarah Frewin
For those of you who don’t know me, I'm Sarah, a Clinical Nurse Specialist in Endocrinology. For the last 7 years I’ve worked with Petros Perros at the Freeman Hospital in Newcastle. I had a fantastic time working with Petros and all you registrars who have happened through the Freeman during my time, but in February last year things changed dramatically for me. I was dispatched by the Trust to do a prescribing course to help me run my clinics in a more efficient way. Over the past few years Petros had tried to encourage me to apply to go to medical school but I had always resisted, not believing that I was bright enough and convincing myself nursing was my lot in life. This course changed my opinion not only of my own abilities but also of nursing in general. One of the tutors on the course made a comment one day that nurses could convert to medicine in four years. I had never appreciated this, and the seed was sown. I spent the next few weeks in turmoil trying to decide whether I should apply or not. For a start I didn’t know whether I would even be accepted or meet the selection criteria. On top of that there were the financial implications of leaving my job and going back to full time study. After a few sleepless nights I eventually broached the subject with Petros hoping he would bring me back to my senses. “Well I told you to do it years ago” were his words and the rest’s a whirlwind. My husband was ecstatic about the idea and vowed to find the money come what may, as I was to be his new pension plan. Before I knew it I was being interviewed for a place in the course at Durham’s Stockton campus.
The interview was quite possibly one of the most emotional experiences I have ever had, not knowing what to expect, what they were looking for and it meaning so much to me. I was interviewed in May of last year and told that I could have a place on the reserve list as all the places were taken. Well I was devastated but not deterred, I vowed to hang on until the A level results came out. A level results came and went but still no news. I began to hound them with daily phone calls and eventually at the end of August the call came to say I had a place. I now know what it must feel like to be a contestant on pop Idol. When I got the call all I could do was say thank you, thank you, thank you. The course leader must have thought I was a blithering idiot!
Knowing what I know now however, the interview was the easy part; it was the first month or so that challenged me more than anything ever before. Anyone who tells you nursing stands you in good stead for medicine is sadly misguided! I spent the first few weeks thinking any day now they’ll teach me something I already know, but alas it was never to be! I truly believed that with ten years nursing and two degrees under my belt it would be a breeze and I would be able to opt out of lots of lessons. Oh how deluded I was!
The first four weeks constituted the ‘Foundation Course’ aimed at getting all students up to the same level in terms of human and cell biology. I didn’t do science at school and nursing tends to skim over these issues. The fact that chromosomes were actually scrunched up DNA was an absolute revelation to me I’m embarrassed to say and don’t get me started on protein folding! So the Foundation Course, which was supposed to be the easy part was one of he most difficult things I've ever done. One of my new friends, Claire was a molecular cell biologist before medical school, spent endless hours with play-dough chromosomes teaching me about mitosis and meiosis. In fact in retrospect within the first few weeks of the course there was nothing that I didn’t struggle with. I never once questioned whether I had made the right decision but did occasionally wonder if I could cut the mustard.
I struggled through the Foundation Course only to be met head on by Cardio Vascular, Respiratory and Renal Medicine (CVRRM). The Foundation Course suddenly paled into insignificance beside it, but at last a session I had been waiting for, measurement of Blood Pressure arrived. One session from which I could at last opt out, however I ended up having to help out as a demonstrator for the rest of the students! Its not all a hard slog, lots of the course is aimed at the more ‘touchy feely’ side of medicine which is right up my street. Lots of the other students are struggling with the social science, research and clinical skills side of things but these come relatively easily to me because of my nursing background and previous degrees. I’ve also discovered an affinity for physiology, which I never expected, perhaps because of the fantastic way it has been taught and the enthusiasm of the teacher.
Well the first exams (formative) were in November and I passed, I’m relieved to say. I didn’t come top of the year by any stretch of the imagination but I was happy with the results and they renewed my self-belief that I really can do it. So I’m sitting here writing this with six days to go until my first proper summative exams, make or break time, hopefully make!
I’d like to take this opportunity to thank all the people who have supported me, encouraged me and kept me calm over the past year. In particular I would like to thank Petros for his unwavering belief in me and all his help with the application forms and interview, I couldn’t have done it without him. Also Raz Nayar for his friendship and encouragement when I was going to give up on applying and since, his time sacrifices in helping me get through my exams.
Roll on the summer holidays, for all of you who have forgotten about the delights of university holidays……. four months off!
RECENT PUBLICATIONS FROM THE NORTHEAST
Please send us your recent publication for inclusion in the next newsletter.
1. Ball SG, Barber T, Baylis PH. Tests of posterior pituitary function. J Endocrinol Invest. 2003;26:15-24.
2. Ball SG, Barber TM. Molecular development of the pancreatic beta cell: implications for cell replacement therapy. Trends Endocrinol Metab. 2003;14:349-55.
3. Dashora U, Mathias D, James A, Zammit-Maempel I, Perros P. Management of recurrent pituitary cysts with pituitary-nasal drain. Pituitary 2003, 5:225-233.
4. Harding S, Greenwood R, Aldington S, Gibson J, Owens D, Taylor R, Kohner E, Scanlon P, Leese G; Diabetic Retinopathy Grading and Disease Management Working Party. Grading and disease management in national screening for diabetic retinopathy in England and Wales. Diabet Med. 2003;20:965-71.
5. Hart RH, Perros P. Glucocorticoids in the medical management of Graves' ophthalmopathy. Minerva Endocrinol. 2003;28:223-31.
6. Hawthorne G, Irgens LM, Lie RT, Moe N, Jervell J. Retraction of paper on maternal diabetes. BMJ. 2003;327:929.
7. Krassas GE, Perros P. Thyroid disease and male reproductive function. J Endocrinol Invest 2003;26:372-380
8. Marshall SM. Inhibition of the renin-angiotensin system: added value in reducing cardiovascular and renal risk? Diabet Med. 2004;21:1-3.
9. Perros P, Mallick UK, Fenwick JD. Radioiodine Uptake in Normal Female Breasts and Liver of a Patient with Differentiated Thyroid Cancer Imaged by Whole Body Scanning. Thyroid 2003; 13, 511.
10. Phillips AW, Fenwick JD, Mallick UK, Perros P. The impact of Clinical guidelines on surgical management of thyroid cancer. Clin Oncol 2003, 15:485-489.
11. Rawling LD, Advani A, Marshall SM, Thomas TH. Neutrophil antigen exposure is altered with age in relatives of patients with Type 2 diabetes. Diabetologia. 2003 Dec 10 [Epub ahead of print]
12. Sibal L, Ugwu P, Kendall-Taylor P, Ball SG, James RA, Pearce SH, Hall K, Quinton R. Medical therapy of macroprolactinomas in males: I. Prevalence of hypopituitarism at diagnosis. II. Proportion of cases exhibiting recovery of pituitary function. Pituitary. 2003;10:243-6.
13. Syed AA, Irving JAE, Redfern CPF, Hall AG, Unwin NC, White M, Bhopal RS, Alberti KGMM, Weaver JU. Low prevalence of the N363S polymorphism of the glucocorticoid receptor in South Asians living in the United Kingdom. Journal of Clinical Endocrinology & Metabolism 2004, 89(1), 232-235
14. Syed AA, Weaver JU. Insulin resistance and coronary artery disease: body mass index may have affected results. Diabetes, Obesity and Metabolism 2004, 6(1), 78
15. Syed AA. Invisible oedema. Journal of the Royal College of Physicians of Edinburgh 2003, 33, 295-296
16. Syed AA. What is a good death?: A good death follows a good life. BMJ 2003, 327(7422),1047
17. Syed AA, Evans C, Ludgate M, Lazarus JH. Early changes in thyroid stimulating antibody activity following radioiodine therapy. Medical Principles and Practice 2003, 12(4), 266-268.
18. Taylor R. Conundrum of the HOPE study: time of taking ramipril may account for lack of relation between blood pressure and outcome. BMJ. 2003;327:681-2
19. Weightman DR, Mallick UK, Fenwick JD, Perros P. Discordant serum thyroglobulin results generated by two classes of assay in patients with thyroid carcinoma: correlation with clinical outcome after 3 years of follow-up. Cancer 2003; 98:41-7.
20. Patel S, Woods DR, Macleod NJ, Brown A, Patel KR, Montgomery HE, Peacock AJ.Angiotensin-converting enzyme genotype and the ventilatory response to exertional hypoxia. Eur Respir J. 2003 Nov;22(5):755-60.
21. Woods D, Sanders J, Jones A, Hawe E, Gohlke P, Humphries SE, Payne J, Montgomery H. The serum angiotensin-converting enzyme and angiotensin II response to altered posture and acute exercise, and the influence of ACE genotype. Eur J Appl Physiol. 2003; 6:821-896.
RECENT PUBLICATIONS IN DIABETES & ENDOCRINOLOGY THAT HIT THE NEWS OR THAT MAY HAVE A SIGNIFICANT IMPACT ON MANAGEMENT
Withdrawal of long-term cabergoline therapy for tumoural and nontumoural hyperprolactinaemia. Colao A, Di Sarno A, Cappabianca P, Di Somma C, Pivonello R, Lombardi G. N Engl J Med. 2003 Nov 20;349:2023-33.
This important observational and prospective trial looked at whether the withdrawal of treatment in patients with nontumouralhyperprolactinaemia, microprolactinomas, or macroprolactinomas is safe and effective. The study population included 200 patients--25 patients with nontumoral hyperprolactinaemia, 105 with microprolactinomas, and 70 with macroprolactinomas. Withdrawal of cabergoline was considered if prolactin levels were normal, magnetic resonance imaging (MRI) showed no tumour (or tumour reduction of 50% or more, with the tumour at a distance of more than 5 mm from the optic chiasm, and no invasion of the cavernous sinuses or other critical areas), and if follow-up after withdrawal could be continued for at least 24 months. Recurrence two to five years after the withdrawal of cabergoline was 24% in patients with nontumoural hyperprolactinaemia, 31% for microprolactinomas and 36% for macroprolactinomas. Renewed tumour growth did not occur in any patient; in 10female patients (22%) and 7 male patients (39%) with recurrent hyperprolactinaemia, gonadal dysfunction redeveloped. In all diagnostic groups, prolactin levels at the time of recurrence were significantly lower than at diagnosis (Pless than 0.001). The Kaplan-Meier estimated rate of recurrence at five years was higher among patients with macroprolactinomas and those with microprolactinomas who had small remnant tumours visible on MRI at the time of treatment withdrawal than among patients whose MRI scans showed no evidence of tumour at the time of withdrawal (patients with macroprolactinomas, 78% vs. 33%, P=0.001; patients with microprolactinomas, 42% vs. 26%, P=0.02). In conclusion, cabergoline can be safely withdrawn in patients with normalised prolactin levels and no evidence of tumour. However, because the length of follow-up in this study was insufficient to rule out a delayed increase in the size of the tumour, it is essential that patients be closely monitored.
The treat-to-target trial: randomised addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patients. Riddle MC, Rosenstock J, Gerich J; Insulin Glargine 4002 Study Investigators.
This randomised, open-label, parallel, 24-week multicentre trial compared the abilities and associated hypoglycaemia risks of insulin glargine and human NPH insulin added to oral therapy of type 2 diabetes to achieve a target HbA1c of 7%. 756 overweight men and women with inadequate glycaemic control (HbA1c more than 7.5%) on one or two oral agents continued their prestudy oral agents and received bedtime glargine or NPH once daily, titrated using a simple algorithm (see table) seeking a target fasting plasma glucose (FPG) less than 5.5 mmol/l.
 The mean FPG at end point was similar with glargine and NPH (6.5 vs. 6.7 mmol/l), as was HbA(1c) (6.96 vs. 6.97%). 60% of patients attained HbA1c less than 7% with each insulin type. However, nearly 25% more patients attained this without documented nocturnal hypoglycaemia (less than 4.0 mmol/l) with glargine (33.2 vs 26.7%, P less than 0.05). Moreover, rates of other categories of symptomatic hypoglycaemia were 21-48% lower with glargine. In conclusion, systematically titrating bedtime basal insulin added to oral therapy can safely target HbA1c in a majority of overweight patients with type 2 diabetes with HbA1cbetween 7.5 and 10.0% on oral agents alone. In doing this, glargine causes significantly less nocturnal hypoglycaemia than NPH, thus reducing a leading barrier to initiating insulin. This simple regimen may facilitate earlier and effective insulin use in routine medical practice, improving achievement of recommended standards of diabetes care.
The mean FPG at end point was similar with glargine and NPH (6.5 vs. 6.7 mmol/l), as was HbA(1c) (6.96 vs. 6.97%). 60% of patients attained HbA1c less than 7% with each insulin type. However, nearly 25% more patients attained this without documented nocturnal hypoglycaemia (less than 4.0 mmol/l) with glargine (33.2 vs 26.7%, P less than 0.05). Moreover, rates of other categories of symptomatic hypoglycaemia were 21-48% lower with glargine. In conclusion, systematically titrating bedtime basal insulin added to oral therapy can safely target HbA1c in a majority of overweight patients with type 2 diabetes with HbA1cbetween 7.5 and 10.0% on oral agents alone. In doing this, glargine causes significantly less nocturnal hypoglycaemia than NPH, thus reducing a leading barrier to initiating insulin. This simple regimen may facilitate earlier and effective insulin use in routine medical practice, improving achievement of recommended standards of diabetes care.NEXT NEWSLETTER Due out beginning of June 2004, so keep the gossip coming.
posted by Arutchelvam at 1:39 PM
![]()
![]()


1 Comments:
do study abroad consultants in hyderabad you want to study in abroad today or in the next intake. we are the best and top rated study abroad consultancies in india with good visa assurance.we help you in filing the f1 visa abroad education consultancy in hyderabad for you in very less time. we are also help you with information needed to apply for the college university.
Post a Comment
<< Home