Endodiabology 2005; Issue 1 (February)
ENDODIABOLOGY
NORTHEAST NEWSLETTER
FOR SPRs AND BOSSES TRAPPED IN THE NORTHERN DEANERY
FEBRUARY 2005
Editors: Shahid Wahid and Petros Perros
Associate Editors: Peter Carey and Freda Razvi
SpR PLACEMENTS (NTN/VTN year of training from 1st October 2004)
RVI- Elin Lim(2), Simon Ashwell(4), Ibrahim M Ibrahim (4), Reena Thomas (3), Freda Razvi (3/4)
Freeman- David Woods(5), Arun(4), Arutchelvan Vijayaraman (3)
North Tyneside/Wansbeck- Vishmawitra Sharma/ Jaysri Ranjani
South Tyneside- Akheel Syed (3)
Gateshead- Olivia Pereira (1/2)
Sunderland- Asghar Madathil (1), Khaled Mansur-Dukhan (1)
North Tees/Hartlepool- Stella Kaddis(5) / Sukesh Chandran (1)
Middlesbrough- Kamal Abouglila(5), Peter Carey(3), Beas Bhatacharya (2)
Carlisle- Isabelle Howat (1)
Bishop Auckland / Durham- / Sony Anthony(3),
NGH/QEH- Subir Ray (1)
Research with numbers (supervisor)- Latika Sibal (Prof Home), Salman Razvi (Dr Weaver), B Ravikumar (Prof Taylor), Sath Nag (Dr Connolly), Mutu Jayapaul (Prof Walker), Ebaa El Ozairi (USA-Prof Home), Andrew Advani (Australia)
MEETINGS / LECTURES / ANNOUNCEMENTS
16th February 2005 Society for Endocrinology Clinical cases meeting, RCP London. Contact Society for Endocrinology
23rd February 2005 Northern Endocrine & Diabetes Winter CME, Freeman Hospital. Contact Simon Ashwell
1st March 2005 7th Clinicopathological Conference on Pituitary Disease, RCPL, London. Contact Cathy Stewart, Tel 01462 459 726.
12th March 2005 Association of Physicians Meeting, Queen Elizabeth Hospital. Contact Roy Taylor .
16th March 2005 Acute Medical Emergencies, RCPL, Freeman Hospital. Contact Lorraine Waugh 0191 223 1247
17th March 2005 1730-2000 28th Novo Nordisk Lecture, Lumley Castle, Durham. Contact Sally Marshall .
23rd March 2005 SpR GIM training ½ day-Freeman Hospital. Contact Contact Lorraine Waugh 0191 223 1247
4th-6th April 2005 British Endocrine Societies Conference 2005, Harrogate. Contact Society for Endocrinology
6th-7th April 2005 ABCD Spring Meeting, Harrogate. Contact P Winocour or ABCD website .
7th-8th April 2005 Insulin Pump Course, JCUH, Middlesbrough. Contact Helen Scales .
20th-22nd April 2005 DUK Annual Professional Conference, SECC, Glasgow. Contact Ben Holdstock or Diabetes UK website .
4th May 2005 (afternoon) NRDSAG and Diabetes Audit meeting. Contact Jola Weaver .
13-14th May 2005 European Diabetic Nephropathy Study Group, Arnhem, Netherlands. Contact Roby Trevisan .
18th May 2005 SpR GIM training ½ day-Sunderland Royal Hospital. Contact Contact Lorraine Waugh 0191 223 1247
26th May 2005 Northern Endocrine & Diabetes Summer CME, Freeman Hospital. Contact Simon Ashwell.
4th-7th June 2005 ENDO 2005, San Diego, USA. Contact ENDO email or ENDO website .
10th-14th June 2005 American Diabetes Association 65th Annual Scientific Sessions, San Diego, USA. Contact ADA email .
4th-8th July 2005 The Society For Endocrinology Summer School, Durham. Contact Simon Pearce or Ann Lloyd
6th July 2005 SpR GIM training ½ day-Freeman Hospital. Contact Lorraine Waugh 0191 223 1247 Lorraine Waugh
TRAINING ISSUES
Record of Internal Training Assessments The RITAs are planned for Thursday the 19th May 2005 and the morning of 20th May 2005. Shaz Wahid is co-ordinating them. If you have not had the information electronically or via the post please contact him. As well as completing the standard documentation Trainees will be asked to submit a structured CV and their agreed aims/objectives for the year with the latter documentation. Important dates to remember are:
Confirm availability for RITA before Monday 14th March 2005
Meet with Educational Supervisor before 22nd April 2005
Send all documentation to Shaz Wahid by 26th April 2005
These are essential dates to adhere to.
Joint Trainers/Trainees meeting the traditional annual get-together will be on Mon 20th June 2005 at the Education Centre, University Hospital of Hartlepool.
Change of circumstances It is essential that all trainees inform the STC via the programme director well in advance of any intentions such as resignation, maternity leave, undertake research, request for an interdeanery transfer, etc. Over the years the STC has been very understanding and bent over backwards to accommodate requests, however with the recent worrying trend that the STC is usually told last, the STC may have to adapt a hard nose approach and apply the 3 month rule or more if applicable.
Regional Endocrine Summer School The Society for Endocrinology Summer School will be hosted by us (Pearce, Ball and James) July 4th to 8th in Durham. There will be a clinical practice day, a molecular endocrinology workshop and the advanced endocrine course. It is a fantastic opportunity for all SpRs and consultants in the region to get local high-quality (cheap) CPD. Please adjust all clinics that week as there will be no SpRs or consultants to do them.
Training Committee Regional Speciality Advisor & Programme Director - Richard Quinton; Committee Chairman - Jola Weaver; Consultant member - Jean Macleod ; Consultant member (RITA Co-ordinator) - Shahid Wahid; Consultant member (Research Advisor) - Simon Pearce; SpR representatives - Simon Ashwell & Andrew Advani.
THE COMMITTEE WOULD LIKE TO ADD AN EXTRA CONSULTANT MEMBER Interested trainers please contact Richard Quinton.
NEW FACES ON THE SCENE
Welcome to Subir Roy, who joins us as a new SpR (with a training number) and is currently in the joint post between the QEH and Newcastle Diabetes Centre.
Welcome to Khaled Mansur-Dukhan, who joins us as a new SpR (with a training number) and is currently at Sunderland Royal.
OLD FACES ON THE GO
Andrew Advani is now in Australia undertaking a period of research. He is due to join the rotation again in October.
NEWS FROM THE NORTHEAST
Freda Razvi has returned from maternity leave.
Simon Pearce has joined the STC as a Consultant Member with the role as Research Advisor for any interested SpRs.
Congratulations to Mark Walker on his appointment to the Diabetes UK board of Trustees.
Congratulations to David Woods on the birth of his baby daughter (Eloise), promotion to Lieutenant Colonel, award of the Mitchiner Medal from the Army Medical Services, appointment as SpR representative on the Clinical Committee of the Society for Endocrinology and the award of his MD with a commendation.
Prof Taylor will be delivering the Arnold Bloom Lecture at this years DUK Annual Professional Conference.
LETTERS
Contributions for this section can include meeting reports, research experiences, book reviews, experiences abroad, and anything else you feel may benefit trainees and trainers around the region. The success of this section really does depend on YOU.
First Teaching EUGOGO course on Graves' orbitopathy-Petros Perros
The European Group On Graves’ Orbitopathy (EUGOGO) came to existence a few years ago aiming to enhance research and education relating to Graves’ eye disease. Newcastle was among the 9 founding centres for this organisation, which is hosting its first educational course due to take place in Thessaloniki, Greece on the 26th and 27th of May 2005. The course will include lectures, interactive sessions and “hands-on” practice in assessing patients. The course is suitable for Endocrinologists both at consultant and SpR level who may wish to enhance their knowledge and skills in managing this condition. The course has been allocated meeting has been awarded 9 European CME credits (ECMEC). Places for the course are restricted, so if you wish to register do so without delay by contacting Prof Krassas telephone: 00-30-2-310-479-633, fax: 00-30-2-310-282-476 & 0-30-23-10-479-633
Message From Bob Peaston-Screening for phaeochromocytoma is best undertaken by obtaining several timed overnight urine samples for catecholamine measurements. Furthermore, plasma metanephrines are a useful addition for the diagnosis of phaeochromocytoma. A proposed strategy for the detection of phaeochromocytoma (Figure)
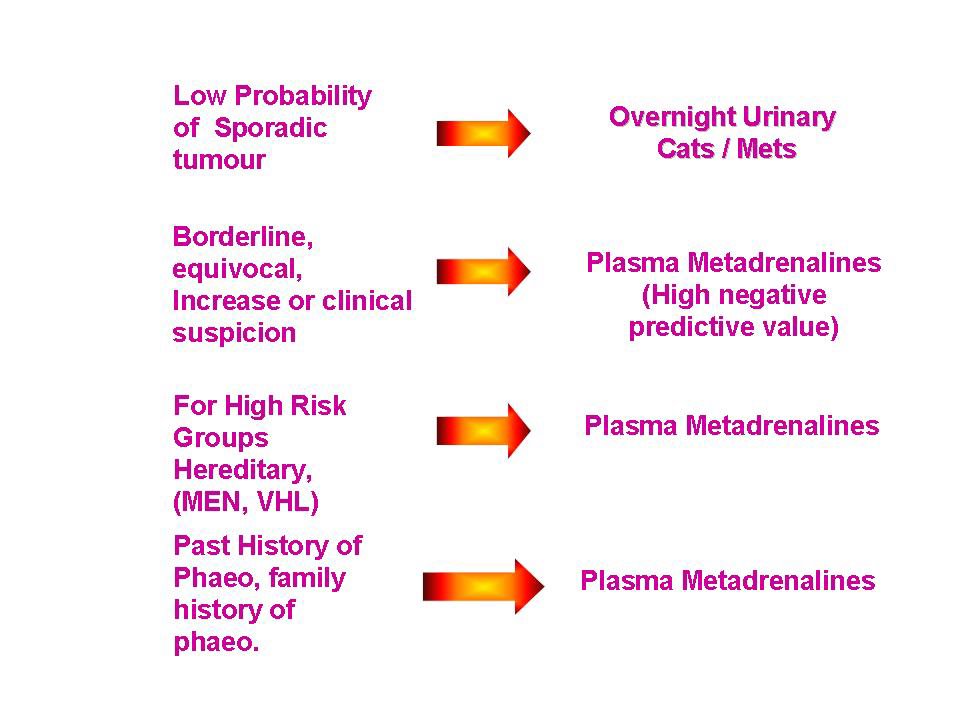 For plasma metadrenalines send 2x5ml EDTA (FBC tube) samples to the Freeman Hospital FAO Bob Peaston, Clinical Biochemistry. For further information please contact Bob Peaston .
For plasma metadrenalines send 2x5ml EDTA (FBC tube) samples to the Freeman Hospital FAO Bob Peaston, Clinical Biochemistry. For further information please contact Bob Peaston .Radio Iodine Training-Shaz Wahid.
An ARSAC certificate can only be obtained by a Consultant Endocrinologist and then it is site specific, limited to treatment of thyrotoxicosis or non-toxic multinodular goitre and renewable after 5 years. For trainees wishing to apply for an ARSAC it is essential to build a portfolio of experience in nuclear endocrine medicine during a 5-year training programme. During each attachment it is essential to get know the medical physicist and ideally if you are in year 5 to arrange several seminars. Things to cover in your portfolio are:
1. Basic principles of radionuclide production, hazards and therapeutic use with emphasis on the management and protection of patients plus the medico-legal implications
2. Administration of Radio-Iodine-witnessing and confirming identification
3. Consenting patients for RAI and explaining therapy
4. Explaining contact restrictions following RAI
5. Follow-up and monitoring post RAI
6. The interpretation of endocrine nuclear imaging-Thyroid technetium scanning, parathyroid subtraction scans (Sestamibi), MIBG, pentetreotide imaging and selenor-cholesterol imaging
The inclusion of any audit/research projects related to nuclear medicine would be a plus point. On appointment to a Consultant post it is important to arrange some local seminars in Nuclear Physics with the Medical Physicist. An ARSAC application can be submitted 6-12 months in to the post. For more information see ARSAC website .
Book Review by Akheel Syed-Endotext.com
The Internet is a wonderful resource for information on anything and everything under the sun and endocrinology is no exception. However, it is not always easy to find trustworthy material without access controls such as paid subscriptions or intrusive advertising. Endotext.com is an online textbook of endocrinology that, try as you may, fails to disappoint. It is a completely free web-based resource sponsored by various pharmaceutical companies but refreshingly does not carry intrusive headline banners, pop-ups or advertising links. Pages are laid out in scrollable frames: the text in a large central frame, hyperlinks to other sections in a vertical frame on the left, and references in a horizontal frame at the bottom(Figure).
 The textbook is organised into several sections covering the major endocrine organs edited by eminent endocrinologists in their fields. The chapters are well-written, well-organised, authoritative, adequately illustrated, provided with hyperlinks to relevant information in other sections in the textbook or reliable outside sources, and superbly referenced. However, the references frame does not provide hyperlinks to the source material – an enhancement that would serve the readers well. The book has a decent Search facility so one can easily home in on a topic of interest.
The textbook is organised into several sections covering the major endocrine organs edited by eminent endocrinologists in their fields. The chapters are well-written, well-organised, authoritative, adequately illustrated, provided with hyperlinks to relevant information in other sections in the textbook or reliable outside sources, and superbly referenced. However, the references frame does not provide hyperlinks to the source material – an enhancement that would serve the readers well. The book has a decent Search facility so one can easily home in on a topic of interest.Verdict: Definitely one for the Favourites/Bookmarks list!!!
Childrens Camps-Stuart Bennett.
Diabetes UK needs individuals (doctors) to volunteer for their Children's Support Holidays and Family Support Weekends for 2005. Time to attend these events can be taken as approved study leave. I would recommend that all trainees in Diabetes & Endocrinology should attend one of these Care Support Events at least once during their specialist training. The relevant parts of the curriculapertaining to these requirements are included below. For further information on volunteering and an application form follow this link:Diabetes UK website
Competence based curricula (after Jan 2003)Section 6, Experience (Additional)17. Attend or speak at meetings of 'lay' patient support organisations.18. Attend a diabetic childrens' camp as a helper.
Curricula (before 1 Jan 2003)6. Management of children and adolescents with diabetes. The trainee must gain experience of management of children with diabetes. This will involve attendance at paediatric diabetic clinics and some exposure to in-patient management. The management of adolescents with diabetes is difficult and demanding. The trainee must acquire experience of this through regular involvement with the care of adolescents. These aspects of training will require close contact with and support from paediatricians. Valuable experience can be gained from involvement in diabetic children's camps and young persons' activity holidays.
RECENT PUBLICATIONS FROM THE NORTHEAST
Please send us your recent publication for inclusion in the next newsletter.
1. Boehm BO, Vaz JA, Brondsted L, Home PD. Long-term efficacy and safety of biphasic insulin aspart in patients with type 2 diabetes. Eur J Intern Med. 2004 Dec;15(8):496-502.
2. Consoli A, Gomis R, Halimi S, Home P, Mehnert H, Strojek K, Van Gaal L. Initiating oral glucose-lowering therapy with metformin in type 2 diabetic patients: an evidence-based strategy to reduce the burden of late-developing diabetes complications. Diabetes Metab. 2004 Dec;30(6):509-16.
3. Dickinson AJ, Vaidya B, Miller M, Coulthard A, Perros P, Baister E, Andrews CD, Hesse L, Heverhagen JT, Heufelder AE, Kendall-Taylor P. Double-blind, placebo-controlled trial of octreotide long-acting repeatable (LAR) in thyroid-associated ophthalmopathy. J Clin Endocrinol Metab. 2004 Dec;89(12):5910-5.
4. Home P, Mbanya JC, Horton E. Standardisation of glycated haemoglobin. BMJ. 2004 Nov 20;329(7476):1196-7.
5. James L, Onambele G, Woledge R, Skelton D, Woods D, Eleftheriou K, Hawe E, Humphries SE, Haddad F, Montgomery H.IL-6-174G/C genotype is associated with the bone mineral density response to oestrogen replacement therapy in post-menopausal women. Eur J Appl Physiol. 2004 92(1-2):227-30.
6. Marshall SM. Recent advances in diabetic nephropathy. Postgrad Med J. 2004 Nov;80(949):624-33.
7. McMillan CV, Bradley C, Woodcock A, Razvi S, Weaver JU. Design of new questionnaires to measure quality of life and treatment satisfaction in hypothyroidism. Thyroid. 2004 Nov;14(11):916-25.
8. Pearce SHS. Spontaneous reporting of adverse reaction to carbimazole and propylthiouracil in the United Kingdom. Clinical Endocrinology 2004: 61; 589-594.
9. Quinton R & Bouloux P-MG. 2004 The management of hypogonadism: a treatment update. Medicine Matters in Secondary Care. Nov 2004. Issue 89.
10. Ravikumar B, Carey PE, Snaar JE, Deelchand DK, Cook DB, Neely RD, English PT, Firbank MJ, Morris PG, Taylor R. Real time assessment of postprandial fat storage in liver and skeletal muscle in health and type 2 diabetes. Am J Physiol Endocrinol Metab. 2004 Nov 30; [Epub ahead of print].
11. Razvi S, Weaver JU. Subclinical hypothyroidism and cardiovascular risk. Thyroid. 2004 Oct;14(10):870; author reply 871-2.
12. Sibal L, Scoones DJ, Bilous R. Temporal arteritis in the absence of headache. Hosp Med. 2004 Nov;65(11):692-3.
13. Singhal P, Caumo A, Cobelli C, Taylor R. Effect of repaglinide and gliclazide on postprandial control of endogenous glucose production. Metabolism. 2005 Jan;54(1):79-84.
14. Smith BR, Bolton J, Young S, Collyer A, Weeden A, Bradbury J, Weightman D, Perros P, Sanders J, Furmaniak J. A new assay for thyrotropin receptor autoantibodies. Thyroid. 2004 Oct;14(10):830-5.
15. Syed AA, Redfern CP, Weaver JU. Aldosterone revisited. N Engl J Med. 2004 Nov 11;351(20):2131-3; author reply 2131-3.
16. Velaga MR, Wilson V, Jennings CE, Owen CJ, Herington S, Donaldson PT, Ball SG, James RA, Quinton R, Perros P, Pearce SHS. The codon 620 tryptophan allele of the lymphoid tyrosine phosphatase (LYP) gene is a major determinant of Graves’ Disease. J Clin Endocrinol Metab. 2004; 89: 5862-65.
17. Warren RE, Perros P, Nyirenda MJ, Frier BM. Serum thyrotropin is a better predictor of future thyroid dysfunction than thyroid autoantibody status in biochemically euthyroid patients with diabetes: implications for screening. Thyroid. 2004 Oct;14(10):853-7.
18. Weaver JU, Razvi S, Bartholomew P. The detrimental effect of anti-thyroid drugs on the outcome of radioiodine therapy is not directly due to decreased radioiodine uptake: Reply. Nucl Med Commun. 2005 Jan;26(1):70.
RECENT PUBLICATIONS IN DIABETES & ENDOCRINOLOGY THAT HIT THE NEWS OR THAT MAY HAVE A SIGNIFICANT IMPACT ON MANAGEMENT
Sjostrom L, Lindroos AK, Peltonen M, Torgerson J, Bouchard C, Carlsson B, Dahlgren S, Larsson B, Narbro K, Sjostrom CD, Sullivan M, Wedel H; Swedish Obese Subjects Study Scientific Group. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004;351:2683-93.
This prospective, controlled study involved obese subjects who underwent gastric surgery and matched with conventionally treated obese control subjects. The follow-up data for subjects (mean age, 48 years; mean body-mass index, 41) who had been enrolled for at least 2 years (4047 subjects) or 10 years (1703 subjects) before the analysis (January 1, 2004) were reported. The follow-up rate for laboratory examinations was 86.6% at 2 years and 74.5% at 10 years. After two years, the weight had increased by 0.1% in the control group and had decreased by 23.4% in the surgery group (P less than 0.001). After 10 years, the weight had increased by 1.6% and decreased by 16.1%, respectively (P less than 0.001). Energy intake was lower and the proportion of physically active subjects higher in the surgery group than in the control group throughout the observation period. Two- and 10-year rates of recovery from diabetes, hypertriglyceridaemia, low levels of high-density lipoprotein cholesterol, hypertension, and hyperuricaemia were more favourable in the surgery group than in the control group, whereas recovery from hypercholesterolaemia did not differ between the groups. The surgery group had lower 2- and 10-year incidence rates of diabetes, hypertriglyceridaemia, and hyperuricaemia than the control group; differences between the groups in the incidence of hypercholesterolaemia and hypertension were undetectable. This study has shown that compared with conventional therapy, bariatric surgery appears to be a viable option for the treatment of severe obesity, resulting in long-term weight loss, improved lifestyle, and, except for hypercholesterolaemia, amelioration in risk factors that were elevated at baseline. Although, not without its faults (non-randomised, non-blinded, the use of several types of surgery and lack of hard end-points) this study has demonstrated the long-term benefits of obesity surgery and now provides some ammunition for those involved in constructing business cases for an obesity service.
Ruggenenti P, Fassi A, Ilieva AP, Bruno S, Iliev IP, Brusegan V, Rubis N, Gherardi G, Arnoldi F, Ganeva M, Ene-Iordache B, Gaspari F, Perna A, Bossi A, Trevisan R, Dodesini AR, Remuzzi G; Bergamo Nephrologic Diabetes Complications Trial (BENEDICT) Investigators. Preventing microalbuminuria in type 2 diabetes. N Engl J Med. 2004;351:1941-51.
This multicenter double-blind, randomized study was designed to assess whether ACE inhibitors and non-dihydropyridine calcium-channel blockers, alone or in combination, prevent microalbuminuria in subjects with hypertension, type 2 diabetes mellitus, and normal urinary albumin excretion. 1204 subjects were randomly assigned to receive at least three years of treatment with trandolapril (at a dose of 2 mg per day) plus verapamil (sustained-release formulation, 180 mg per day), trandolapril alone (2 mg per day), verapamil alone (sustained release formulation, 240 mg per day), or placebo. The target blood pressure was 120/80 mm Hg. The primary end point was the development of persistent microalbuminuria (overnight albumin excretion, more than or =20 microg per minute at two consecutive visits). The primary outcome was reached in 5.7% of the subjects receiving trandolapril plus verapamil, 6.0% of the subjects receiving trandolapril, 11.9% of the subjects receiving verapamil, and 10.0% of control subjects receiving placebo. The estimated acceleration factor (which quantifies the effect of one treatment relative to another in accelerating or slowing disease progression) adjusted for predefined baseline characteristics was 0.39 for the comparison between verapamil plus trandolapril and placebo (P=0.01), 0.47 for the comparison between trandolapril and placebo (P=0.01), and 0.83 for the comparison between verapamil and placebo (P=0.54). Trandolapril plus verapamil and trandolapril alone delayed the onset of microalbuminuria by factors of 2.6 and 2.1, respectively. Serious adverse events were similar in all treatment groups. In subjects with type 2 diabetes and hypertension but with normoalbuminuria, the use of trandolapril plus verapamil and trandolapril alone decreased the incidence of microalbuminuria to a similar extent. The effect of verapamil alone was similar to that of placebo.
Barnett AH, Bain SC, Bouter P, Karlberg B, Madsbad S, Jervell J, Mustonen J; Diabetics Exposed to Telmisartan and Enalapril Study Group. Angiotensin-receptor blockade versus converting-enzyme inhibition in type 2 diabetes and nephropathy. N Engl J Med. 2004;351:1952-61
Tthis prospective, multicenter, double-blind, five-year study randomly assigned 250 subjects with type 2 diabetes and early nephropathy to receive either the angiotensin II-receptor blocker telmisartan (80 mg daily, in 120 subjects) or the ACE inhibitor enalapril (20 mg daily, in 130 subjects). The primary end point was the change in the glomerular filtration rate (determined by measuring the plasma clearance of iohexol) between the baseline value and the last available value during the five-year treatment period. Secondary end points included the annual changes in the glomerular filtration rate, serum creatinine level, urinary albumin excretion, and blood pressure; the rates of end-stage renal disease and cardiovascular events; and the rate of death from all causes. After five years, the change in the glomerular filtration rate was -17.9 ml per minute per 1.73 m2 of body-surface area, where the minus sign denotes a decrement, with telmisartan (in 103 subjects), as compared with -14.9 ml per minute per 1.73 m2 with enalapril (in 113 subjects), for a treatment difference of -3.0 ml per minute per 1.73 m2 (95 percent confidence interval, -7.6 to 1.6 ml per minute per 1.73 m2. The lower boundary of the confidence interval, in favour of enalapril, was greater than the predefined margin of -10.0 ml per minute per 1.73 m2, indicating that telmisartan was not inferior to enalapril. The effects of the two agents on the secondary end points were not significantly different after five years. Telmisartan is not inferior to enalapril in providing long-term renoprotection in persons with type 2 diabetes. These findings do not necessarily apply to persons with more advanced nephropathy, but they support the clinical equivalence of angiotensin II-receptor blockers and ACE inhibitors in persons with conditions that place them at high risk for cardiovascular events. The above 2 studies provide clear evidence that ACE inhibition is just as effective as Angiotensin receptor blockade in delaying the progression of renal dysfunction and microalbuminuria in diabetic nephropathy, although the “gold” standard would be comparative studies with hard end-point morbidity/mortality data. Furthermore, what is required are good quality study comparing dual blockade with single blockade in terms of renal function and protein excretion.
NEXT NEWSLETTER Due out beginning of June 2005, so keep the gossip coming.
posted by Arutchelvam at 3:10 PM
![]()
![]()


{kind=link}
1 Comments:
Who knows where to download XRumer 5.0 Palladium?
Help, please. All recommend this program to effectively advertise on the Internet, this is the best program!
Post a Comment
<< Home